Once a source of national pride, Cuba’s healthcare system declines as energy shortages deepen crisis, writes ANDREA RODRIGUEZ

Austerity, abandonment and assisted dying in Canada
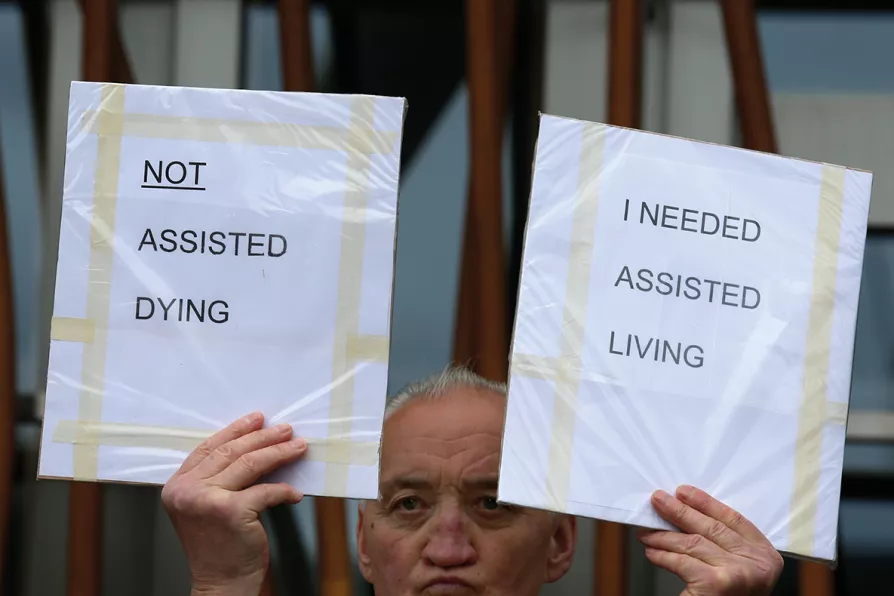
The right to ‘die with dignity’ is warped by austerity and social exclusion, argues JOHN CLARKE

By making it simpler to support workers in struggle, Strike Map’s new Solidarity Fund aims to strengthen strikes when they need it most, write ROBERT POOLE and HENRY FOWLER
ANSELM ELDERGILL explains why the rule of law is fundamental to our liberty and welfare
Only an ambitious programme of state-led investment can restore growth and improve living standards, argues MICHAEL BURKE
Thousands of remarkable Britons left ordinary lives behind to join the struggle against Franco. Here is a snapshot of those who answered the call
The present drive to war is a cynical and deliberate diversion from deteriorating living standards, argues MATT KERR






THE notion that someone facing a terminal illness or fatal condition should be able to decide at what point their life should be brought to a close, and to opt for “death with dignity,” isn’t one that can be brushed aside.
Many of us will find ourselves or someone we love in a situation where such a decision is anything but an abstract consideration.
Yet the reality is that no public policy can be considered outside of the broader social and political context. As austerity measures take ever-greater effect and the provision of healthcare and vital support services are effectively rationed, the danger is that assisted dying can be effectively forced on those who have been socially abandoned.

Similar stories

With more people dying each year and many spending their final days in institutions, researchers argue that wider access to palliative care could offer a more humane and cost-effective alternative, write ROX MIDDLETON, LIAM SHAW and MIRIAM GAUNTLETT

Evidence to peers from medical leaders, patient safety officials and the children’s commissioner has intensified fears that the Bill’s safeguards are inadequate, writes ADAM JAMES POLLOCK


A new report from the Citizens Advice destroys the government narrative about disabled people ‘choosing’ not to work, showing the £3,000 annual cuts will create a two-tiered system based on claim dates rather than needs, writes DYLAN MURPHY