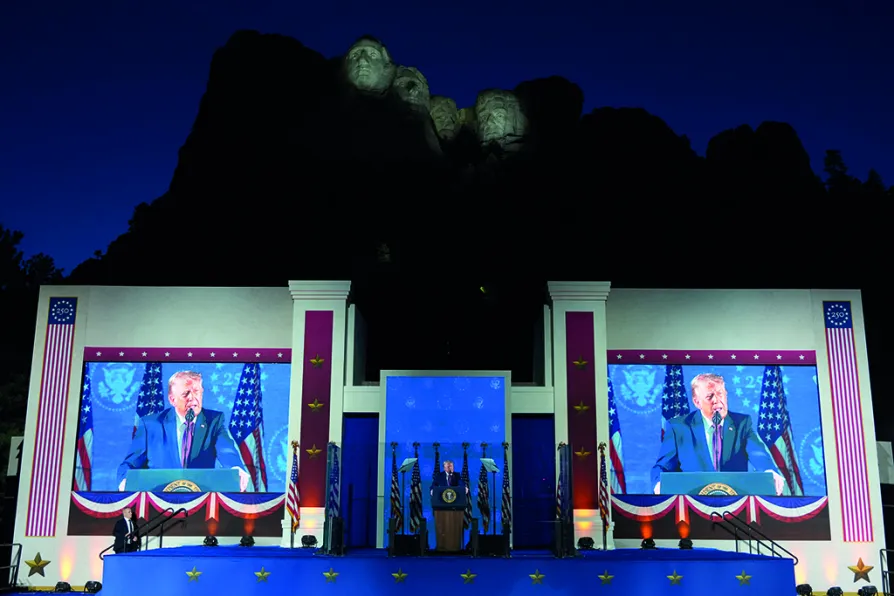
CJ ATKINS takes a closer look at Trump’s recent spate of red-baiting speeches and asks why the authoritarian president is running scared

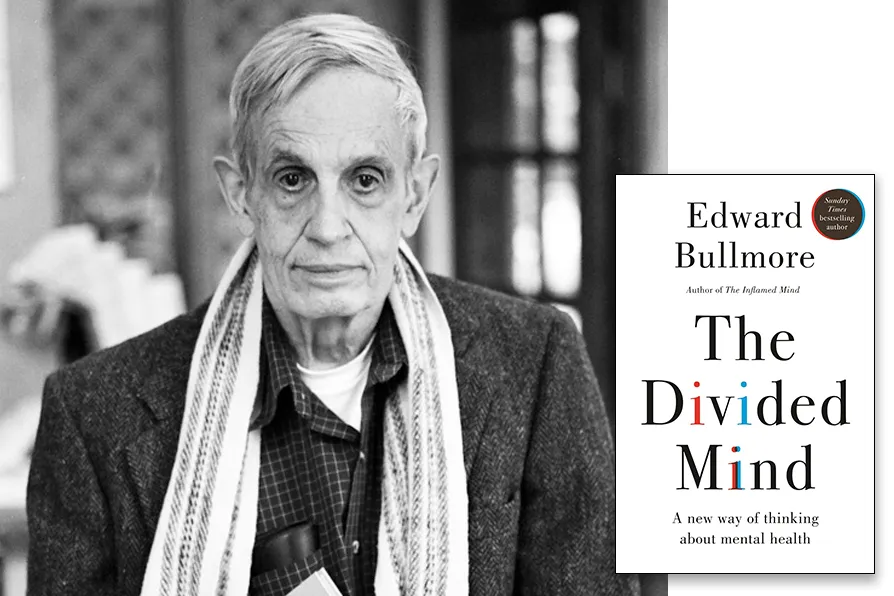
The ‘power threat meaning framework’ – an alternative to diagnosis?
Is the diagnostic model for bipolar disorder too restrictive – and is it helping patients with mental ill health, asks RUTH F HUNT

JOHN McINALLY sees little chance of change at Westminster, and calls on the left to get serious about building a real alternative
With the centenary of the UN Slavery Convention upon us, ROGER McKENZIE argues much needs to be done to rid us of all its contemporary manifestations
SEVIM DAGDELEN says European Nato states are escalating ever closer to direct conflict with a nuclear power, and sacrificing welfare states built up over a century to finance it
CLAUDIA WEBBE says the horrific price British patients will pay for this NHS deal is now clear — and there’s time to get out of it, if MPs will only force the issue
KENNY MacASKILL says the lines between party, government and Civil Service in Scotland have been blurred and we need a thorough investigation into how






WHEN the programme Being Bipolar, with psychotherapist Philippa Perry, was first aired on Channel 4 in 2015, the audience got a taste of anti-psychiatry in practice.
Prior to meeting any patients, Perry spoke about her doubts as to the validity of the diagnosis bipolar. When she met them, she asked whether a traumatic incident in their past had contributed to their condition and led to the symptoms they were experiencing.
One patient swept his arm through the air, and said: “Zero, zero, zero.”

Similar stories
RICHARD SHILLCOCK examines an enjoyable, but philosophically conventional book, and urges Marxists to employ their capacity to embrace the totality in any explanation

Evidence to peers from medical leaders, patient safety officials and the children’s commissioner has intensified fears that the Bill’s safeguards are inadequate, writes ADAM JAMES POLLOCK

1943-2025: How one man’s unfinished work reveals the lethal lie of ‘colour-blind’ medicine
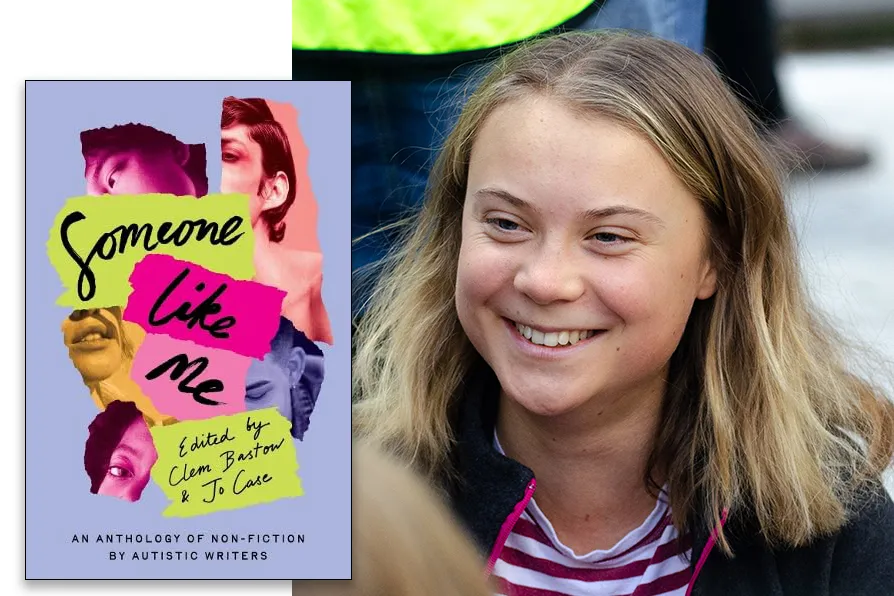
JOSEPHINE BARBARO welcomes a diverse anthology of experiences by autistic women that amounts to a resounding chorus, demanding to be heard