PCS general secretary FRAN HEATHCOTE explains why opposing war is inseparable from defending jobs, wages and public services – and why readers should come to the London Peace Conference on Saturday June 20

The legacy of colonialism in treating ‘sleeping sickness’
A new drug is showing promise for an old disease — but elimination will require more than pharmaceuticals, explain ROX MIDDLETON, LIAM SHAW and JOEL HELLEWELL


As protests erupt over Henry Nowak’s murder, ANDREW MURRAY argues that anger is being exploited to advance a wider racist and anti-immigration agenda
CARLOS MARTINEZ explains the sound case for car manufacturing co-operation with China
The National Emergency Briefing outlines the need for urgent action to address environmental crisis, says PAUL DONOVAN, warning that there’s no time to indulge the arguments of the fossil-fuel-funded climate-change deniers
Campaigners say criticism of Labour MP Stephen Morgan’s position on Gaza has been met with police intervention and cancelled opportunities for debate. HESTER WOLFE reports
The Committee for the Defence of Iranian People’s Rights warns of escalation danger in Iran war






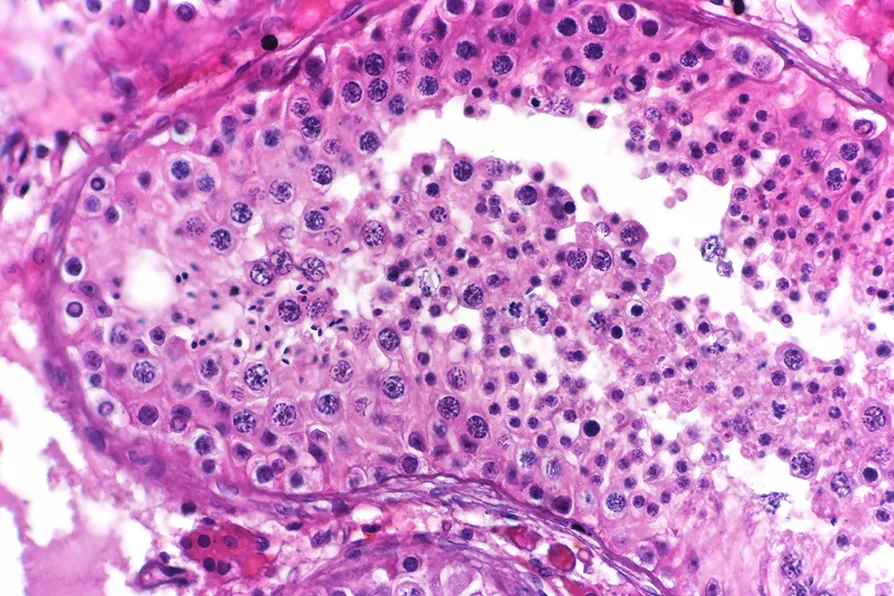
HUMAN African trypanosomiasis, abbreviated as HAT, is a potentially fatal disease caused by infection with a parasite, Trypanosoma brucei. The parasite is transmitted between humans via the bite of the tsetse fly. When a tsetse fly carrying parasites bites a person, the parasitic cells enter the person’s blood. There, the parasite’s cells start to divide into two and multiply.
This initial “blood stage” infection can cause non-specific symptoms such as fever, headaches, and joint pains. These general symptoms are difficult to diagnose as trypanosomiasis. Proper diagnosis requires looking at blood that has been treated with a special staining chemical under a microscope so that the parasite cells stand out.
This lack of easily noticeable symptoms has meant that many HAT cases go undetected. This is particularly concerning because, left untreated, chronic blood-stage infections will progress to the “neurological stage.” This is when the parasites cross the blood-brain barrier and infect the brain and spinal fluid.
When the parasites progress to the brain they cause much more severe symptoms such as muscle weakness, tremors, and confusion. Infected individuals also experience very disturbed sleeping patterns, leading to the common nickname of “sleeping sickness” for HAT cases. People’s experiences include insomnia, bouts of sudden sleepiness during the day, or a totally reversed sleeping pattern, where they are awake all night and feel sleepy all day.
The neurological stage also produces psychological changes in the host, producing emotional instability and psychosis. Left untreated, it will eventually lead to death. Unfortunately, once the parasites have crossed the blood-brain barrier, treatment is more difficult.
Treatment of late-stage HAT involves drug delivery over the course of 10 days in hospital, which is often not possible for people in rural locations where the disease is most likely to have gone untreated. The drugs for the neurological stage are also more toxic with greater side effects.
Though diseases like HAT and malaria had existed in tropical regions for a long time, colonialism worsened them by increasing the movement of workers between tropical regions and port cities, cramming people together. One epidemic in Uganda beginning in 1901 raged for 20 years, killing an estimated 200,000 people.

Similar stories

With more people dying each year and many spending their final days in institutions, researchers argue that wider access to palliative care could offer a more humane and cost-effective alternative, write ROX MIDDLETON, LIAM SHAW and MIRIAM GAUNTLETT
New research into mutations in sperm helps us better understand why they occur, while debunking a few myths in the process, write ROX MIDDLETON, LIAM SHAW and MIRIAM GAUNTLETT

Politicians who continue to welcome contracts with US companies without considering the risks and consequences of total dependency in the years to come are undermining the raison d’etre of the NHS, argues Dr JOHN PUNTIS
ALEX DITTRICH hitches a ride on a jaw-dropping tour of the parasite world