The greatest threat to democracy may no longer come from political parties but from unelected tech oligarchs like Peter Thiel and his powerful Silicon Valley network, argues JOHN GREEN

The practice of FGM has to be eradicated
Government cuts and a lack of commitment to the ethos of public health are allowing the abuse of girls and women to continue unchecked, writes HILARY BURRAGE


Today’s interconnected conflicts are enriching the arms industry while pushing the entire world towards permanent militarisation, argues ROGER McKENZIE
by Nana Backland, Merseyside Morning Star Readers & Supporters Group
The government’s Pip review looks like a carefully managed exercise in legitimising future cuts to disability support, argues Dr DYLAN MURPHY
The Tories introduced the 50% strike ballot threshold to make industrial action harder. MATT WRACK argues that a Labour government has no justification for leaving it on the statute book






SOMETIMES events come together in a propitious manner; and so it is with the first ever successful prosecution in Britain for female genital mutilation, just days before the date today when people around the globe declare zero tolerance of FGM.
Within a few days, both Britain and the world have shown a determination that FGM must become history — but sadly declarations do not necessarily equate to outcomes.
The “reasons” why FGM has not been eradicated already are many. Most nations around the globe now have legislation against FGM, explicitly or, as for instance in the case of France (where, as also in Kenya and some other countries, dozens of successful prosecutions have been achieved), implicit.

Similar stories
The legacy of socialist feminists such as Alexandra Kollontai challenges us today to confront an uncomfortable truth: framing prostitution as empowerment lets the abusers of the Epstein class off the hook, warns HELEN O’CONNOR

AMANDA J QUICK warns about the ever-expanding influence of the sex industry – and the harm it unleashes on both the women involved and society collectively, especially the young

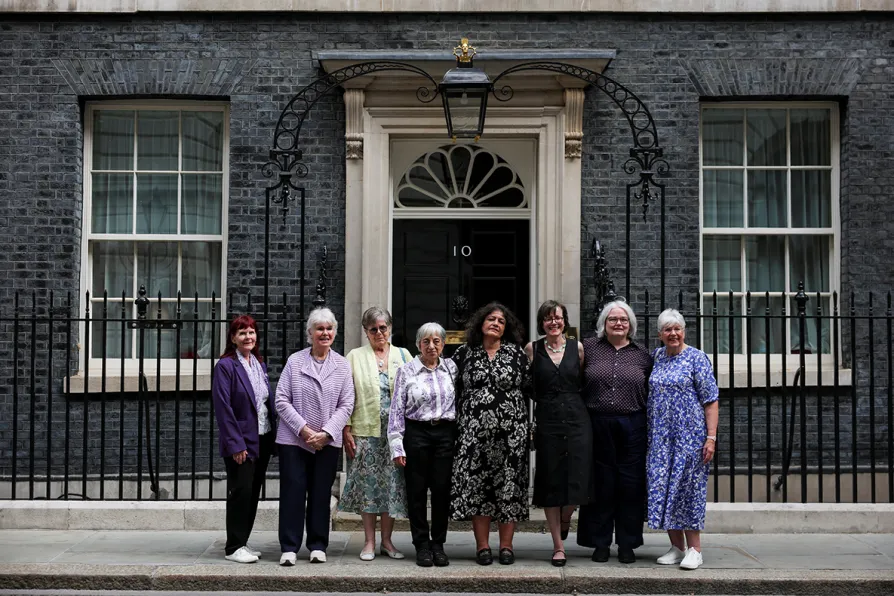
LYNNE WALSH reports from the Women’s Declaration International conference on feminist struggles from Britain to the Far East